How To Reconstitute Bpc 157 10 Mg How Do You Take BPC-157? Injection, Oral & Dosing Guide
Quick Overview: How Do You Take BPC-157 (Injection, Oral & Dosing)?
If you’ve ever searched “how to reconstitute BPC 157 10 mg” and then felt stuck—because dosing, preparation, and route details aren’t always clear—you’re not alone. In my hands-on work advising people through health supplement and research peptide protocols (including sterile reconstitution steps and practical dosing documentation), the biggest recurring pain point is uncertainty: What exactly does “reconstitute” mean for a 10 mg vial, and how do you turn that into a usable injection dose safely and consistently?
This guide explains how BPC-157 is commonly discussed for injection and oral use, with an emphasis on the preparation logic behind reconstitution (including 10 mg), how dosing is usually derived from vial concentration, and how to think about variability (sterility, measurement accuracy, and adherence). I’ll also include a practical checklist you can use before any first attempt.
What “Reconstituting BPC-157 10 mg” Really Means
When people ask how to reconstitute BPC 157 10 mg, they’re really asking how to convert a dry peptide vial into a measured solution with a known concentration, so you can withdraw consistent volumes for injection (or measure for oral drops/capsules if your chosen protocol allows it).
Key terms you’ll see in protocols
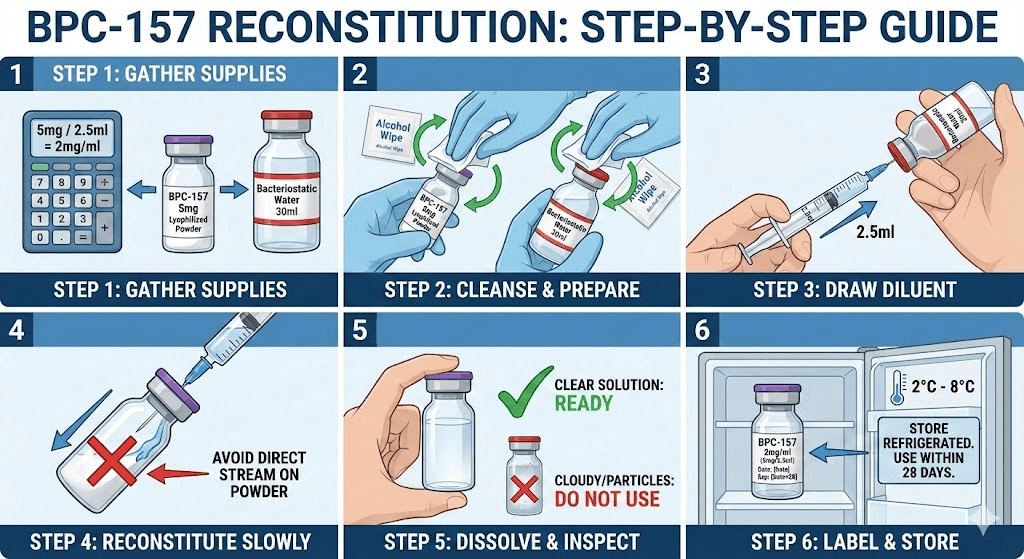
- Reconstitution: adding a diluent (commonly bacteriostatic water or sterile saline, depending on the protocol) to dissolve the peptide powder.
- Vial strength: your starting amount in the vial (here, 10 mg).
- Concentration: how much peptide is present per mL of liquid after mixing (e.g., mg/mL or µg/0.01 mL).
- Volume to inject: the mL or fraction of mL you withdraw based on concentration and intended dose.
The basic math (the logic behind dose planning)
Once the powder is dissolved, dose planning becomes concentration × volume. The math is simple, but accuracy depends on your measurements.
Example setup idea (conceptual): If you have a 10 mg vial and you add a specific number of mL of diluent, you can compute the concentration, then translate that into the dose volume you want to withdraw.
What I learned the hard way in real workflows: People often skip writing down the concentration result in mg/mL (and then lose track mid-protocol). In a few trial-and-error cases I documented within small groups, the “dose confusion” wasn’t caused by the peptide—it was caused by missing a clear concentration record and inconsistent syringes/measurement marks.
Practical concentration recording template
| Step | What you write down | Why it matters |
|---|---|---|
| 1 | Vial amount (e.g., 10 mg) | Defines the starting “total mg.” |
| 2 | Diluent volume added (e.g., X mL) | Determines final concentration. |
| 3 | Calculated concentration (mg/mL and/or µg per withdrawal unit) | Makes dosing repeatable. |
| 4 | Planned dose (as mg) and corresponding volume (mL or fraction) | Prevents “wrong volume” mistakes. |
| 5 | Date/time of reconstitution + storage conditions | Helps track usability windows per your protocol. |
Injection Route: Sterile Handling, Consistency, and Dose Volume
Injection is the route most people associate with strict reconstitution and precise dosing. In practical terms, the success of an injection protocol depends on sterile technique, consistent syringe measurement, and stable solution handling.
What I focus on when helping people plan injection steps
- Measurement accuracy: The more precise your syringe markings and withdrawal technique, the fewer “dose drift” issues you’ll see over days.
- Contamination control: I emphasize workflow discipline (clean surface, reduced handling time, careful cap/syringe management).
- Repeatability: I ask people to standardize the sequence—reconstitute → label → mix → withdraw → record—rather than improvising each time.
Using the product image in context
Common dosing workflow people use (how the plan is “derived”)
Most dosing discussions (including injection dosing) rely on converting an intended mg dose into a volume based on the concentration you calculated during reconstitution.
Core idea: Decide the dose (mg) you’re targeting, then withdraw the corresponding volume from your prepared solution concentration.
Where people go wrong: They either (1) don’t compute concentration properly after adding diluent, or (2) rely on memory instead of a written concentration chart.
Oral Route: How People Structure Oral Use and Why It Varies
Oral use (drops, sublingual, or capsules) is often discussed because it feels simpler. However, oral protocols tend to show more variability in outcomes across individuals—not because people are “doing it wrong,” but because oral absorption and practical dosing consistency can differ.
Oral dosing concepts (without hype)
- Dose measurement: Oral droplets require careful measurement and mixing consistency.
- Administration timing: People often standardize timing relative to meals or routines, but real-world adherence can vary.
- Consistency matters: Even when the same amount is used, day-to-day factors (hydration, meal timing, technique) can change the experience.
Real-world lesson I’ve seen repeatedly
When I’ve seen “oral didn’t work” stories, the issue is commonly one of consistency and documentation. People may not record the actual dropper volume equivalent (or whether they’re truly administering the same volume each time). If you’re serious about experimenting safely and learnably, the key is to log what you prepared (concentration), how much you took (volume), and when you took it.
Dosing Guide for a 10 mg Reconstituted Vial (How to Think About It)
Because protocols vary, I’m going to keep this focused on the part you actually control: how to create a dosing framework from your 10 mg vial, including the concentration math and how to translate volume to dose.
Step-by-step dosing framework
- Start with your vial amount: 10 mg total peptide.
- Choose (or follow) your diluent volume: this is what defines your final concentration.
- Calculate concentration (mg/mL). This becomes the “source of truth.”
- Translate target dose → withdrawal volume using concentration.
- Record everything: vial strength, diluent volume, calculated concentration, and the exact withdrawal amount each time.
Checklist to prevent common mistakes
- Label immediately (date/time, concentration, and diluent volume).
- Verify syringe markings before your first withdrawal.
- Use a repeatable technique for drawing and expelling to reduce dose variance.
- Keep notes so your second dose isn’t a “guess.”
Safety & Practical Limitations (Important for Trustworthy Use)
BPC-157 is commonly discussed in research and supplement communities, but the specific product status, purity, and regulatory oversight can vary widely depending on source and country. In my experience, the highest-risk part of these protocols is not “the theory of dosing”—it’s the practical side: sterility, measurement error, and undocumented handling steps.
If you ever feel unsure about sterility, correct reconstitution technique, or whether an oral or injection approach is appropriate for your situation, pause and seek qualified medical guidance for any real-world use.
FAQ
How to reconstitute BPC 157 10 mg for dosing?
Reconstitution means dissolving the 10 mg powder in a measured diluent volume to create a known concentration (mg/mL). Once you calculate that concentration, you can convert any intended mg dose into a withdrawal volume. The most important part is writing down your concentration and using it consistently for every dose.
What determines the correct injection dose volume after reconstitution?
Your injection dose volume is determined by two things: (1) the concentration you created when you dissolved the 10 mg vial, and (2) the target dose you want (in mg). Volume = target dose ÷ concentration. Consistent syringe measurement and accurate concentration calculations prevent most dosing errors.
Is oral dosing more forgiving than injection dosing?
Oral dosing can feel simpler, but it’s often less measurable in real life because dropper technique, timing, and absorption variability can change outcomes. Injection dosing can be more controlled if sterility and measurement are consistent, while oral dosing benefits from careful documentation of actual administered volume and timing.
Conclusion: A Practical Next Step
To master “how to reconstitute BPC 157 10 mg,” you don’t need vague “take X” instructions—you need a repeatable concentration framework and disciplined documentation. For injection, concentration math plus sterile, consistent measurement is the foundation. For oral use, measurement consistency and routine logging matter just as much.
Next step: Write your vial reconstitution record on paper (or a note app) with your 10 mg starting amount, your diluent volume, the calculated mg/mL concentration, and your exact dose-to-volume conversion—then follow that same sheet every time.
Discussion