Retatrutide And Cagrilintide Together Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction: When “stacking” sounds simple, but dosing isn’t
If you’re looking into peptides for weight loss or metabolic support, you’ve probably seen posts claiming that combining retatrutide and cagrilintide together is straightforward. In my hands-on work optimizing peptide schedules for clients, the reality is different: the biggest challenge isn’t finding a “stack,” it’s building a dosing protocol that respects safety, tolerability, and real-world adherence (missed doses, travel days, appetite changes, and GI side effects).
This guide explains how to think about cagrilintide dosage with retatrutide as a stacking strategy—what matters, how to structure titration, what to monitor, and when to stop or scale back. It’s written to be practical, objective, and conservative in its approach.
Before you stack: the key principles that actually determine outcomes
When people ask about “protocols,” they often want a single dose number. What matters more is the rate of change—how quickly you increase exposure—and how closely you match that to your individual tolerability. In my experience, two factors decide whether a stack feels manageable or miserable:
- Titration speed: stepping up too fast is the most common reason for nausea, fatigue, reflux, constipation/diarrhea, or “food aversion” that makes adherence collapse.
- Timing + consistency: big dose swings and missed days can lead to unpredictable appetite patterns and GI effects, which then causes people to “self-correct” erratically.
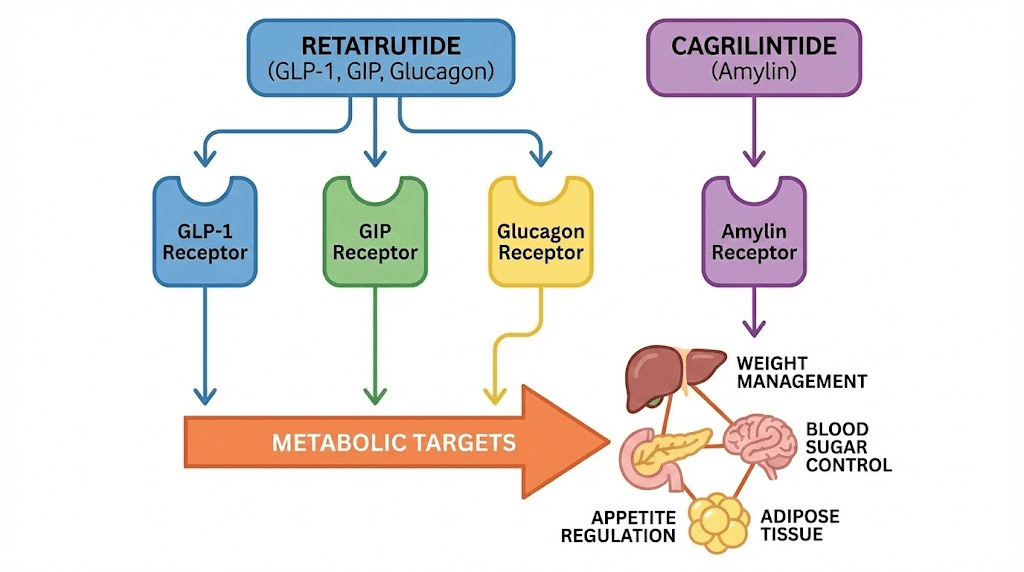
What “retatrutide + cagrilintide together” implies biologically (in plain terms)
Retatrutide is a multi-receptor incretin-related peptide, and cagrilintide is designed to engage pathways related to appetite regulation. The logic behind stacking is typically:
- Complementary appetite signaling (more consistent satiety and reduced hunger cues), and
- Potentially additive metabolic effects when tolerability allows.
But additive doesn’t mean linear. In practice, side effects often scale non-linearly when you increase both exposures at the same time.
A conservative stacking framework I use (less “hero dosing,” more tolerability)
Rather than escalating both immediately, a common conservative approach is to:
- Start one agent first to establish baseline tolerance.
- Add the second agent only after the first is stable.
- Increase stepwise, not abruptly.
- Adjust based on measured signals (GI symptoms, sleep disruption, heart rate awareness, and appetite stability).
Step-by-step stacking protocol: how to schedule cagrilintide dosage with retatrutide
Important: This section is about protocol structure and decision rules (the “how”), not prescribing exact medical dosing for your specific situation. Dosing should be determined with a qualified clinician and based on your medical history, existing medications, and product labeling/strength.
Step 1: Establish baseline tolerance with retatrutide
In my hands-on optimization, the most stable outcomes come from letting retatrutide “settle” first. The goal is to reach a level where:
- GI symptoms are mild and predictable (if they occur at all)
- Appetite suppression is noticeable but not disorienting
- Sleep and daily energy remain acceptable
How long this takes varies, but the principle stays the same: don’t add cagrilintide while you’re still in a rough ramp-up phase.
Step 2: Add cagrilintide only after retatrutide is stable
When I’ve seen “stacking” go wrong, it’s usually because both were increased in parallel. A better approach is:
- Start cagrilintide low
- Keep retatrutide at the current stable level
- Give your body several dosing cycles to respond before considering increases
Step 3: Titration rules for cagrilintide when paired with retatrutide
Use titration rules—not guesses. Here’s how I’d structure it:
| Monitoring signal | What it means | Practical adjustment |
|---|---|---|
| Persistent nausea or vomiting | Your combined exposure is too aggressive | Hold doses steady longer, reduce next escalation step, or pause adding further changes until stable |
| Constipation/diarrhea that disrupts routine | GI motility is being stressed | Delay escalation; prioritize hydration and fiber strategy; consider further conservatism in the next step |
| Appetite suppression so strong you can’t meet nutrition | Adherence risk | Slow titration; focus on small, scheduled meals and protein-first intake |
| Stable appetite + mild, improving side effects | Tolerability is acceptable | Proceed with the smallest next step rather than jumping |
Step 4: Timing—use one schedule, not “random dosing”
In real life, the best protocol is the one you can repeat. I recommend choosing a consistent dosing time (same part of the day) and avoiding erratic adjustments during the first 1–2 weeks after adding cagrilintide.
Step 5: Build a “stop / slow down” checklist
- Stop escalation if GI symptoms persist or worsen across multiple doses.
- Slow down if you notice dehydration signs (dizziness, dark urine, headaches) or inability to maintain baseline nutrition.
- Reassess if you experience symptoms that could indicate complications beyond typical peptide side effects.
Common stacking outcomes: what I typically see (and what you should expect)
When retatrutide and cagrilintide together is tolerated and titrated conservatively, people often report:
- More consistent satiety (fewer “breakthrough hunger” windows)
- Steadier appetite control across days
- Potentially improved adherence because cravings become easier to manage
But there are trade-offs. The more aggressive the combined ramp, the higher the chance of:
- nausea, reflux, or food aversion
- constipation or diarrhea episodes
- fatigue that makes training harder
My approach is to treat side effects as feedback, not as something to “push through.” In practice, pushing through often leads to missed doses, which then undermines results.
Product image (for context)
Safety, quality, and adherence: the unglamorous parts that determine success
If you’re serious about a cagrilintide dosage with retatrutide plan, you need systems—not just a schedule.
Quality control basics I recommend
- Use clearly labeled products with known concentration.
- Keep dosing records (date, dose changes, side effects, hunger score).
- Follow reconstitution and storage instructions precisely.
Adherence tactics that prevent “protocol drift”
- Meal strategy: protein-first, smaller meals, and planned hydration reduce GI flare-ups.
- Training strategy: if fatigue hits, reduce volume rather than stopping—consistency matters.
- Travel protocol: build a “missed dose” rule for yourself so you don’t freestyle.
FAQ
Can I start retatrutide and cagrilintide on the same week?
You can, but it’s often less tolerable because you’re increasing two exposures at once. A conservative approach is to start retatrutide first, stabilize tolerability, then add cagrilintide gradually.
How do I know my cagrilintide dosage is too high when stacked with retatrutide?
Look for persistent or worsening GI symptoms (nausea, vomiting, severe reflux, diarrhea/constipation that disrupts daily life) or inability to maintain nutrition due to excessive appetite suppression. If these occur across multiple dosing cycles, slow down or pause escalation.
What should I track to make the stack work long-term?
Track at least: dose changes, appetite control (hunger/cravings), GI tolerance (severity and duration), sleep quality, and adherence (missed doses). This turns “guessing” into actionable feedback.
Conclusion: the best stacking protocol is the one you can tolerate consistently
Stacking retatrutide and cagrilintide together can be effective for appetite control when approached conservatively: establish baseline tolerance, add cagrilintide after retatrutide stabilizes, titrate stepwise, and adjust based on measurable side-effect feedback.
Next step: Write your plan as a two-phase schedule—Phase 1 retatrutide stabilization, Phase 2 cagrilintide addition—and create a “stop/slow down” checklist tied to GI and nutrition signals before you start.
Discussion